
Page 94 - Remedial Andrology
P. 94
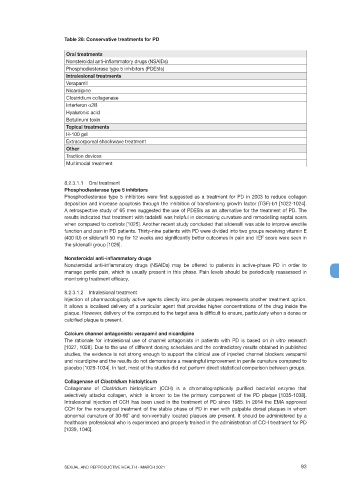
Table 26: Conservative treatments for PD
Oral treatments
Nonsteroidal anti-inflammatory drugs (NSAIDs)
Phosphodiesterase type 5 inhibitors (PDE5Is)
Intralesional treatments
Verapamil
Nicardipine
Clostridium collagenase
Interferon α2B
Hyaluronic acid
Botulinum toxin
Topical treatments
H-100 gel
Extracorporeal shockwave treatment
Other
Traction devices
Multimodal treatment
8.2.3.1.1 Oral treatment
Phosphodiesterase type 5 inhibitors
Phosphodiesterase type 5 inhibitors were first suggested as a treatment for PD in 2003 to reduce collagen
deposition and increase apoptosis through the inhibition of transforming growth factor (TGF)-b1 [1022-1024].
A retrospective study of 65 men suggested the use of PDE5Is as an alternative for the treatment of PD. The
results indicated that treatment with tadalafil was helpful in decreasing curvature and remodelling septal scars
when compared to controls [1025]. Another recent study concluded that sildenafil was able to improve erectile
function and pain in PD patients. Thirty-nine patients with PD were divided into two groups receiving vitamin E
(400 IU) or sildenafil 50 mg for 12 weeks and significantly better outcomes in pain and IIEF score were seen in
the sildenafil group [1026].
Nonsteroidal anti-inflammatory drugs
Nonsteroidal anti-inflammatory drugs (NSAIDs) may be offered to patients in active-phase PD in order to
manage penile pain, which is usually present in this phase. Pain levels should be periodically reassessed in
monitoring treatment efficacy.
8.2.3.1.2 Intralesional treatment
Injection of pharmacologically active agents directly into penile plaques represents another treatment option.
It allows a localised delivery of a particular agent that provides higher concentrations of the drug inside the
plaque. However, delivery of the compound to the target area is difficult to ensure, particularly when a dense or
calcified plaque is present.
Calcium channel antagonists: verapamil and nicardipine
The rationale for intralesional use of channel antagonists in patients with PD is based on in vitro research
[1027, 1028]. Due to the use of different dosing schedules and the contradictory results obtained in published
studies, the evidence is not strong enough to support the clinical use of injected channel blockers verapamil
and nicardipine and the results do not demonstrate a meaningful improvement in penile curvature compared to
placebo [1029-1034]. In fact, most of the studies did not perform direct statistical comparison between groups.
Collagenase of Clostridium histolyticum
Collagenase of Clostridium histolyticum (CCH) is a chromatographically purified bacterial enzyme that
selectively attacks collagen, which is known to be the primary component of the PD plaque [1035-1038].
Intralesional injection of CCH has been used in the treatment of PD since 1985. In 2014 the EMA approved
CCH for the nonsurgical treatment of the stable phase of PD in men with palpable dorsal plaques in whom
abnormal curvature of 30-90˚ and non-ventrally located plaques are present. It should be administered by a
healthcare professional who is experienced and properly trained in the administration of CCH treatment for PD
[1039, 1040].
SEXUAL AND REPRODUCTIVE HEALTH - MARCH 2021 93