
Page 99 - Remedial Andrology
P. 99
increases endothelial nitric oxide synthase (eNOS) and α-smooth muscle actin, given their role in the
pathogenesis of PD [1083]. Only one clinical study assessed the efficacy of VED therapy in mechanically
straightening the penile curvature of PD as monotherapy and further investigation is needed [1084].
8.2.3.1.4 Multimodal treatment
There are some data suggesting that a combination of different oral drugs can be used for treatment of the
acute phase of PD. However, there does not seem to be a consensus on which drugs to combine or the
optimum drug dosage; nor has there been a comparison of different drug combinations.
A long-term study assessing the role of multimodal medical therapy (injectable verapamil associated
with antioxidants and local diclofenac) demonstrated that it is efficacious to treat PD patients. The authors
concluded that combination therapy reduced pain more effectively than verapamil alone, making this specific
combination treatment more effective compared to monotherapy [1083]. Furthermore, combination protocols
including injectable therapies, such as CCH, have been studied in controlled trials. The addition of adjunctive
PTT and VED has been described; however, limited data are available regarding its use [1085].
Penile traction therapy has been evaluated as an adjunct therapy to intralesional injections with interferon,
verapamil, or CCH [1030, 1086, 1087]. These studies have failed to demonstrate significant improvements
in penile length or curvature, with the exception of one subset analysis identifying a 0.4 cm length increase
among men using the devices for > 3 hours/day [1087]. A meta-analysis demonstrated that men who used
PTT as an adjunct to surgery or injection therapy for PD had, on average, an increase in stretched penile length
(SPL) of 1 cm compared to men who did not use adjunctive PTT. There was no significant change in curvature
between the two groups [1088].
Data available on the combined treatment of CCH and the use of VED between injection intervals
have shown significant mean improvements in curvature (-17˚) and penile length (+0.4 cm) after treatment.
However, it is not possible to determine the isolated effect of VED because of a lack of control groups [1047,
1088].
Recent data have suggested that combination of PDE5I (sildenafil 25 mg twice daily) after CCH
treatment (shortened protocol combined with VED) is superior to CCH alone for improving penile curvature and
erectile function. Further studies are necessary to externally validate those findings.
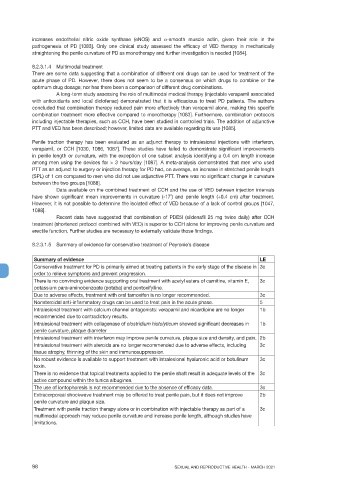
8.2.3.1.5 Summary of evidence for conservative treatment of Peyronie’s disease
Summary of evidence LE
Conservative treatment for PD is primarily aimed at treating patients in the early stage of the disease in 3c
order to relieve symptoms and prevent progression.
There is no convincing evidence supporting oral treatment with acetyl esters of carnitine, vitamin E, 3c
potassium para-aminobenzoate (potaba) and pentoxifylline.
Due to adverse effects, treatment with oral tamoxifen is no longer recommended. 3c
Nonsteroidal anti-inflammatory drugs can be used to treat pain in the acute phase. 5
Intralesional treatment with calcium channel antagonists: verapamil and nicardipine are no longer 1b
recommended due to contradictory results.
Intralesional treatment with collagenase of clostridium histolyticum showed significant decreases in 1b
penile curvature, plaque diameter
Intralesional treatment with interferon may improve penile curvature, plaque size and density, and pain. 2b
Intralesional treatment with steroids are no longer recommended due to adverse effects, including 3c
tissue atrophy, thinning of the skin and immunosuppression.
No robust evidence is available to support treatment with intralesional hyaluronic acid or botulinum 3c
toxin.
There is no evidence that topical treatments applied to the penile shaft result in adequate levels of the 3c
active compound within the tunica albuginea.
The use of iontophoresis is not recommended due to the absence of efficacy data. 3c
Extracorporeal shockwave treatment may be offered to treat penile pain, but it does not improve 2b
penile curvature and plaque size.
Treatment with penile traction therapy alone or in combination with injectable therapy as part of a 3c
multimodal approach may reduce penile curvature and increase penile length, although studies have
limitations.
98 SEXUAL AND REPRODUCTIVE HEALTH - MARCH 2021