
Page 86 - Remedial Andrology
P. 86
7. LOW SEXUAL DESIRE AND MALE
HYPOACTIVE SEXUAL DESIRE DISORDER
7.1 Definition, classification and epidemiology
It has always been a challenge to define sexual desire properly because it has a complicated nature and it
th
can be conceptualised in many different ways. According to the International Classification of Diseases 10
edition (ICD-10), lack or loss of sexual desire should be the principal problem and no other sexual problems
accompanying it such as ED [923]. In the Diagnostic and Statistical Manual of Mental Disorders (DSM-V), male
hypoactive sexual desire disorder (HSDD) is defined as “the persistent or recurrent deficiency (or absence) of
sexual or erotic thoughts or fantasies and desire for sexual activity”. The judgment of deficiency is made by the
clinician, taking into account factors that affect sexual functioning, such as age and general and socio-cultural
contexts of the individual’s life [200]. According to the fourth International Consultation on Sexual Medicine
(ICSM), the definition of male HSDD was proposed as a “persistent or recurrent deficiency or absence of
sexual or erotic thoughts or fantasies and desire for sexual activity (clinical principle)” [924]. Although the
exact prevalence of low sexual desire (LSD) is unknown, a prevalence of 4.7% was reported in a survey of a
population-based sample of middle-aged German men (n = 12,646) [925].
7.2 Pathophysiology and risk factors
Several aetiological factors are considered to contribute to the pathophysiology of LSD. Levine proposed
three components of sexual desire as drive (biological), motivation (psychological) and wish (cultural) [926].
However, it is believed that both in the surveys and clinical practice those three components are usually found
interwoven [927].
7.2.1 Psychological aspects
The endorsement of negative thoughts during sexual intercourse (i.e., concerns about erection, lack of erotic
thoughts, and restrictive attitudes toward sexuality) predicts LSD in men [928]. Furthermore, feeling shame
during sexual intercourse, because of negative sexual thoughts (e.g., concern about achieving erection),
characterises men with LSD as opposed to women with the same condition [929]. Psychological models
testing the interplay role between biopsychosocial factors reveal that reduced male sexual desire is best
predicted by negative thoughts and emotions during sex, more than general psychopathological symptoms or
age [930-932]. Similarly, low confidence achieving erection, no attraction towards their partner, living in long-
term relationships, and stress resulting from work are predictors of LSD in men [933]. In contrast, relationship
factors such as marital satisfaction, cohesion or display of affection receive little support [928, 933]. Even so,
it is worth noting that, despite LSD being less common in men than in women [924], it is the most frequent
complaint in couples’ therapy [934]. Therefore, the role of relationship factors cannot be completely ruled out.
In addition, anxiety proneness has been associated with LSD in men and is expected to shift men’s attention
from erotic cues to worrying thoughts, thereby decreasing sexual desire [935].
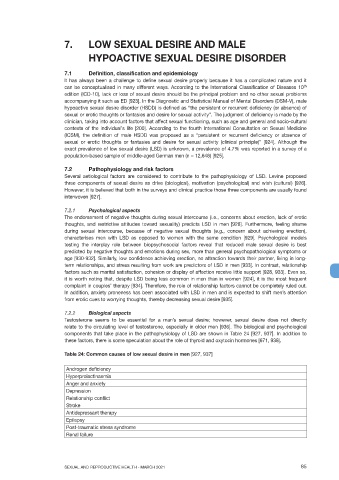
7.2.2 Biological aspects
Testosterone seems to be essential for a man’s sexual desire; however, sexual desire does not directly
relate to the circulating level of testosterone, especially in older men [936]. The biological and psychological
components that take place in the pathophysiology of LSD are shown in Table 24 [927, 937]. In addition to
these factors, there is some speculation about the role of thyroid and oxytocin hormones [671, 938].
Table 24: Common causes of low sexual desire in men [927, 937]
Androgen deficiency
Hyperprolactinaemia
Anger and anxiety
Depression
Relationship conflict
Stroke
Antidepressant therapy
Epilepsy
Post-traumatic stress syndrome
Renal failure
SEXUAL AND REPRODUCTIVE HEALTH - MARCH 2021 85