
Page 82 - Remedial Andrology
P. 82
6.7.2 Pathophysiology and risk factors
Primary anorgasmia is defined as starting from a man’s first sexual intercourse and lasts throughout his
life, while for secondary anorgasmia patients should have a normal period before the problem starts [893].
Substance abuse, obesity and some non-specific psychological aspects, such as anxiety and fear, are
considered risk factors for anorgasmia. Only a few studies have described anorgasmia alone and generally it
has been considered as a symptom linked to ejaculatory disorders especially with DE, and therefore, they are
believed to share the same risk factors. However, psychological factors are considered to be responsible for
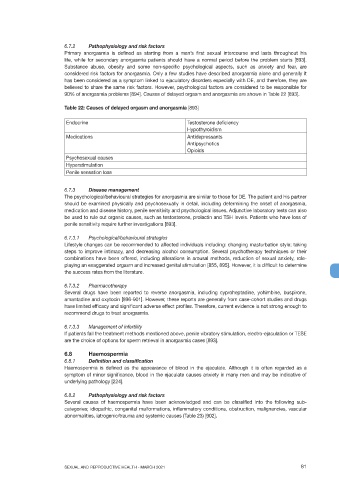
90% of anorgasmia problems [894]. Causes of delayed orgasm and anorgasmia are shown in Table 22 [893].
Table 22: Causes of delayed orgasm and anorgasmia [893]
Endocrine Testosterone deficiency
Hypothyroidism
Medications Antidepressants
Antipsychotics
Opioids
Psychosexual causes
Hyperstimulation
Penile sensation loss
6.7.3 Disease management
The psychological/behavioural strategies for anorgasmia are similar to those for DE. The patient and his partner
should be examined physically and psychosexually in detail, including determining the onset of anorgasmia,
medication and disease history, penile sensitivity and psychological issues. Adjunctive laboratory tests can also
be used to rule out organic causes, such as testosterone, prolactin and TSH levels. Patients who have loss of
penile sensitivity require further investigations [893].
6.7.3.1 Psychological/behavioural strategies
Lifestyle changes can be recommended to affected individuals including: changing masturbation style; taking
steps to improve intimacy, and decreasing alcohol consumption. Several psychotherapy techniques or their
combinations have been offered, including alterations in arousal methods, reduction of sexual anxiety, role-
playing an exaggerated orgasm and increased genital stimulation [855, 895]. However, it is difficult to determine
the success rates from the literature.
6.7.3.2 Pharmacotherapy
Several drugs have been reported to reverse anorgasmia, including cyproheptadine, yohimbine, buspirone,
amantadine and oxytocin [896-901]. However, these reports are generally from case-cohort studies and drugs
have limited efficacy and significant adverse effect profiles. Therefore, current evidence is not strong enough to
recommend drugs to treat anorgasmia.
6.7.3.3 Management of infertility
If patients fail the treatment methods mentioned above, penile vibratory stimulation, electro-ejaculation or TESE
are the choice of options for sperm retrieval in anorgasmia cases [893].
6.8 Haemospermia
6.8.1 Definition and classification
Haemospermia is defined as the appearance of blood in the ejaculate. Although it is often regarded as a
symptom of minor significance, blood in the ejaculate causes anxiety in many men and may be indicative of
underlying pathology [224].
6.8.2 Pathophysiology and risk factors
Several causes of haemospermia have been acknowledged and can be classified into the following sub-
categories; idiopathic, congenital malformations, inflammatory conditions, obstruction, malignancies, vascular
abnormalities, iatrogenic/trauma and systemic causes (Table 23) [902].
SEXUAL AND REPRODUCTIVE HEALTH - MARCH 2021 81